The importance of behaviour change in health interventions
In this blog post from Katie Angotti, Health Coach Lead for our project, she describes how three different behaviour change theories can help achieve the desired behaviour changes in the Bump2Baby and Me Health Coaching Programme.
What is behaviour change?
Behaviour change is exactly as it sounds – the practice of changing people’s behaviour, individually or as a collective. In the context of public health, the goal is to increase the practice of health-promoting behaviours while decreasing or eliminating those that have a negative impact on health.
Behaviour change is rooted in theories and models developed through research and practice that influence practitioners’ decisions when designing and delivering health interventions. These frameworks typically define the stages of a person’s behaviour change journey. Those stages, however, are unique to each person’s life and are heavily influenced by individual factors such as switching jobs or starting a family. A well-designed health intervention draws on the relevant behaviour change theory to guide people through these stages to achieve the desired outcome.
Behaviour change models
The behaviour change frameworks which inform the health coaching approach used within Bump2Baby and Me, include the Transtheoretical model, Social Cognitive Theory, and Self Determination Theory. With this blog post we have described how three different theories can help achieve the desired behaviour changes.
Transtheoretical Model
The Transtheoretical, or Stages of Change, Model is commonly used in health interventions. It is broken down into 6 unique stages:
- Precontemplation:
- Contemplation:
- Preparation:
- Action:
- Maintenance
- Termination
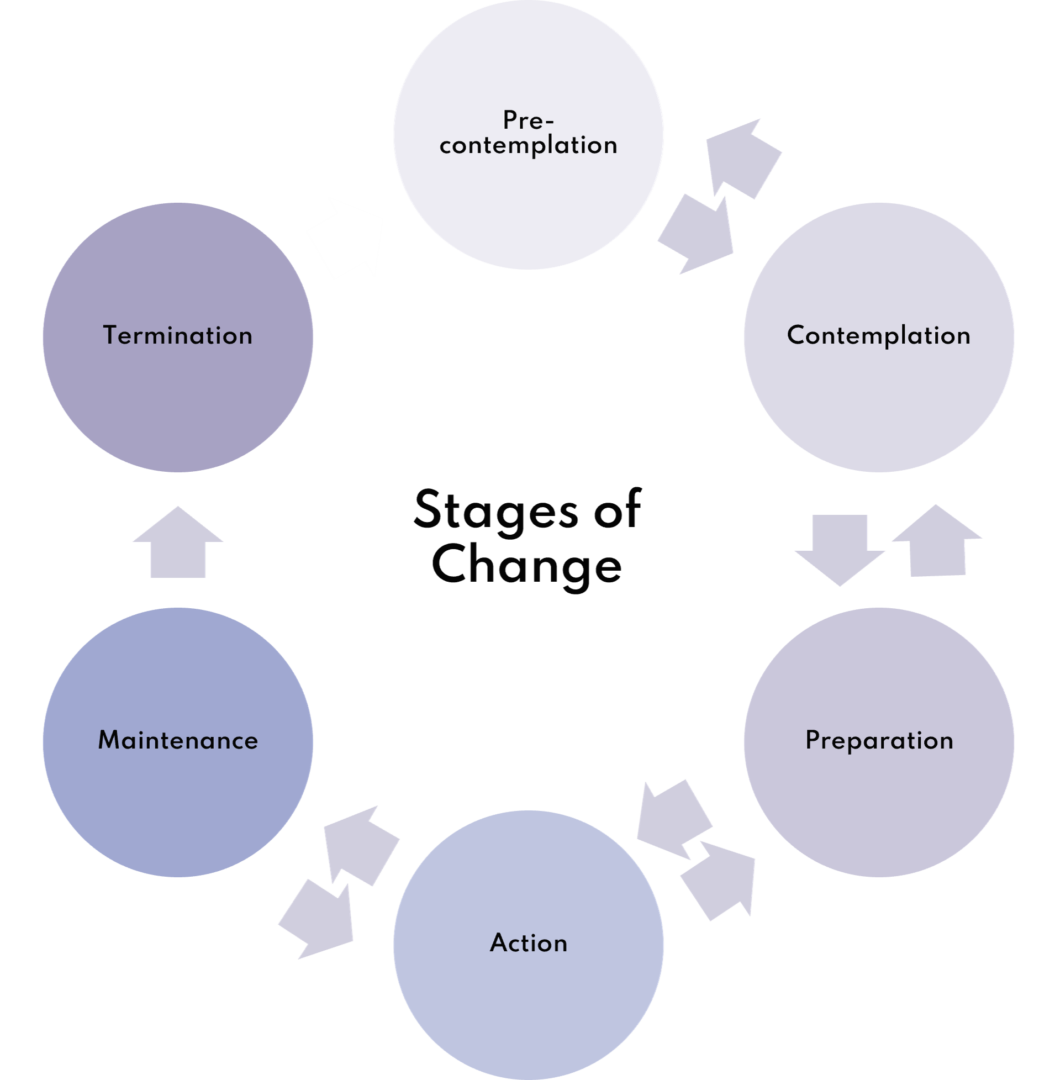
A person may move back and forth between stages multiple times before getting to the maintenance phase, and reaching the termination stage may not always be possible.
Social Cognitive Theory (SCT)
According to SCT, we are primarily driven by external rather than internal forces, resulting from the interaction of personal, environmental, and behavioural factors. For example, a teenager who goes to a party and notices that the people who are drinking alcohol are slurring their speech and being more argumentative and louder than those who are not drinking alcohol. The teenager therefore decides not to drink alcohol to avoid these undesirable effects. SCT acknowledges that multiple variables, such as self-efficacy (the belief that we can achieve influence over the conditions that affect our lives), outcome expectations, and emotional coping (regulating your feelings and emotional response to the problem instead of addressing the problem), can intervene in the process of behaviour change.
An important goal in health interventions is to increase someone’s confidence and belief in themselves to carry out the new behaviour. This is called self-efficacy. Self-efficacy has been shown to influence physical and mental health, learning and achievement, career and job satisfaction and family relations. Depending on the type of intervention, this could entail breaking down tasks into small steps to increase a person’s confidence in their ability to achieve change, rather than overwhelming them with the entire task at the outset.
Self Determination Theory
Self Determination Theory (SDT) integrates human motivation, personality, and optimal functioning to drive behaviour change. SDT recognises that both extrinsic (external) and intrinsic (internal) factors influence a person’s motivation over time, but motivation must be self-determined to sustain a behaviour change.
Using behaviour change theory in interventions
Using a behaviour change framework can help us design more effective health interventions – without this, people may lack motivation and remain in the early stages of an intervention.
Taking the Stage of Change Model as an example, if someone is in the contemplation phase, they are weighing up the pros and cons of the behaviour change – moving straight into action without spending time to address these adequately, making a clear plan and setting realistic goals, is likely to result in the person not achieving the goal and becoming demotivated by the idea of change. An effective intervention should also recognise that people may move backwards as they reach different challenges throughout their behaviour change journey. Life and human behaviour is not predictable, and not all eventualities can be adequately planned for. An intervention that does not recognise and plan for supporting people to move back and forth between stages is not setting them up for success.
Behaviour change theory in Bump2Baby and Me
In relation to the Bump2Baby and Me project, prior to signing up, someone may be at the precontemplation stage – they are not considering making any changes to their lifestyle. Contemplation occurs when their inclusion in the higher risk category for gestational diabetes prompts them to consider a lifestyle change as beneficial. At this stage, they receive information to help them weigh the pros and cons of changing, for example, a factsheet on the health benefits of eating more fibre in pregnancy.
During their first meeting, the health coach guides their client into the preparation phase – identifying any barriers and motivations, making a plan, and defining the next steps by setting SMART goals.
Someone moves into action phase when they start putting those changes into place, and as they work to prevent relapse, they move into the maintenance phase. In a journey like pregnancy, new barriers and challenges may appear at any stage, for example an increase in back and hip pain in later pregnancy may prevent someone from continuing with their goal to run three times a week, and so they need to move back into preparation, adapt the goal to be more suitable and return to the action phase. It should not be a static process.
Behaviour change is a lifelong process, and most people will always be engaged in some kind of behaviour change.
Behaviour change techniques in action
A multidisciplinary team carefully planned the Bump2Baby and Me health programme to ensure that our health coaches applied this theoretical framework and its active components, the behaviour change techniques (BCTs), appropriately. We created a thorough coach handbook that serves not only as training tool but also as a first step towards fidelity assessment (assessing whether the intervention was delivered as intended) and coach evaluation, which are frequently absent in behaviour change interventions’ reports. Therefore, we are currently working on a manuscript that will explore this matter.