Using multiple implementation research methods: the key to unlocking new insights in maternal and child health
Research is a tricky business. You need to know what you’re looking for and choose the best available methods to find out what lies behind the door of the data that you collect. Bump2Baby and Me is using a variety of implementation science methods that will hopefully unlock new knowledge. The types of information being collected requires special types of research methods. Here we outline some of the methods that we’re using in Bump2Baby and Me.
EPIS
EPIS is a model or framework that we used to plan out how we were going to gather the study data on implementation.
- E stands for exploration, which is the initial stage where we examined what is the lie of the land.
- P stands for preparation, which is where the project gathered information on how ready we were to start the project.
- I stands for implementation and this is where the study or the intervention is commenced and completed.
- S stands for sustainment, which is where we will look to see if the intervention is still being used after the active phase has finished.
Overall, this framework provides a good foundation to how an intervention gets planned, delivered, and evaluated when you want to understand how it operates in the real world.
Template for Intervention Description and Replication (TIDieR)
TIDieR is a checklist and guideline developed to help to improve completeness in the reporting of interventions in research studies. It is used to quantify and evaluate the type of things that have happened during an intervention to say whether or not it has been successfully delivered. This framework is widely used in implementation science. The 12 item TIDieR checklist (below) can be adapted for use when planning a study evaluation.
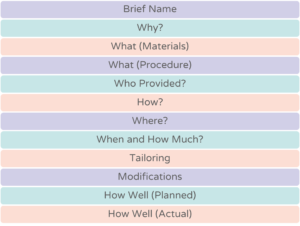
Bump2Baby and Me uses the TIDieR checklist and guideline to ensure we are measuring the important elements that make up the study effect. Using the checklist also allows for comparability between similar studies.
Fidelity
The fidelity evaluation is all about seeing how well an intervention is delivered. This is critical because if we don’t know how well something is delivered, we can’t roll it out in the wider community or scale it up to a bigger intervention. The type of fidelity information that we’re collecting in Bump2Baby and Me is spread throughout the trial. For the standardised screening we are doing in maternity hospitals, we will be looking at how well the screening was performed in each of the study sites. We’re also doing checks on the training of the health coaches to see whether or not they met the required standards over time. We will examine how this worked during the initial intensive training phase and during the additional training that occurred while delivering the study.
We also review how well women engaged with the app to see whether or not there were any differences there. Finally we will look at a broader evaluation, which will have a qualitative component as well. Within the app itself, we will explore how well women interact with the synchronous (in real time) coaching compared with the asynchronous (not in real time) coaching. We will look at what the participant experience was like, where possible including the woman’s partner in order to understand the impact on the family unit. Equally we will examine the experience of the health coaches and wider research staff being involved in the study.
Health economics
Health economics analysis of Bump2Baby and Me will include two different approaches. The first approach will focus on the cost to maternity services and whether or not the study delivered good value for money in preventing complications associated with gestational diabetes and having high levels of gestational weight gain. The second approach will concentrate on the costs to the health service and to the mother. These costs will be calculated during the 12 months of the study after the baby is born.
Quality of life will be used as a core measure within the health economics analysis as well as things like cost diaries and information from medical records that will allow us to cost the complications associated with having higher risk pregnancies. Performing health economics analysis in both pregnancy and the postpartum period will give a more accurate picture that can be used by decision-makers and policymakers in supporting the best outcomes for mother and baby that are also cost effective.
All of these rich pieces of data will fit together to give us a more accurate picture of how the study was implemented and how it potentially could be rolled out or scaled up in the future.